
Accelerated Ageing: What Does That Actually Mean?

I recently saw a post on social media (it has its uses) that referenced a June 2026 article on the U.S.News website entitled Accelerated Aging May Explain Rising Cancer Risk In Young Adults, which begins with the comment that,
“Younger generations have a higher risk of developing cancer earlier in their lives, and a new study advances one potential explanation.”
I was curious to know what that ‘potential explanation’ might be, although I was also doubtful about the possibility that it might reveal the true nature of ‘disease’ and cancer in particular. My doubt is based on what I’ve learned during the course of my two decades of research about the mainstream medical system, and the fact that it does not operate from an understanding of how the body truly functions. That system also fails to acknowledge the role of what I refer to as the ‘non-physical’ aspects of health, by which I mean the mental, emotional, psychological and spiritual aspects of our being. Our health status does not solely rely on on the ‘physical’.
The U.S.News article cites a study entitled Biological aging and generational shifts in early-onset cancer risk that had been published in the journal Nature a few days earlier.
This is not the first time the topic of ‘biological ageing’ has been studied in the medical literature, although it’s not a term I’d paid much attention to before - so I decided to look into it and find out more.
I also wanted to discover the basis of the claim that there’s a rising ‘cancer risk’ in young adults who should represent the healthiest demographic; so why is their ‘risk’ of cancer increasing? I have my own ideas about the reason for this situation that I’ll share later in this article.
The Nature article begins with the statement that,
“Over the past three decades, early-onset cancers, diagnosed in adults often under age 50 or 55 years, have become a global cancer prevention and public health challenge. Between 1990 and 2019, cancers diagnosed under the age of 50 years increased by 24% globally and continue to rise.”
We have to wonder at what point cancer researchers will start to realise that their current strategy just isn’t working! After all, the ‘War on Cancer’ was initiated in 1971 by Richard Nixon. But it has failed abysmally to make any positive impact because the incidence of the ‘disease’ has continued to increase in the intervening 55 years. It is now predicted that 1 in 3 women and 1 in 2 men will be diagnosed at some point in their lifetime with cancer, which is said to be one of the leading causes of death worldwide.
The Nature article provides examples of the situation and states,
“In Australia, Canada, the United Kingdom (UK) and the US, people born in the 1990s face at least a fourfold higher risk of early-onset colorectal cancer compared with those born in the 1960s.”
This is a massive rise in ‘risk’ in the space of only 3 decades. Furthermore, people born in the 1990s are significantly younger than 50.
A similar news release article, published on the website of the AACR (American Association for Cancer Research) in 2024 and entitled Accelerated Aging May Increase the Risk of Early-onset Cancers in Younger Generations, refers to presentations at the 2024 Annual Meeting of the AACR, and specifically to a statement by Ruiyi Tian, a graduate student,
“Multiple cancer types are becoming increasingly common among younger adults in the United States and globally. Understanding the factors driving this increase will be key to improve the prevention or early detection of cancers in younger and future generations.”
She explains the difference between chronological ageing and biological ageing as follows,
“Unlike chronological age, biological age may be influenced by factors such as diet, physical activity, mental health, and environmental stressors,”
These ‘factors’ are similar, but not identical, to those of the WHO. I would have thought they’d be the same; after all, the WHO is the ‘health authority’ for all WHO member countries. I’m aware that that the US is no longer a WHO member, but it was in 2024 when that article was published.
Although not entirely incorrect as factors that can adversely affect our health, the idea that tobacco use, alcohol consumption, unhealthy diet, physical inactivity and air pollution are ‘risk factors’ for cancer is a woefully inadequate explanation for the continual rise in the incidence of cancer.
I would add that the reference to ‘infections’ as a risk factor is totally inappropriate - there is no evidence that any ‘germ’ is the cause of any ‘disease’, including cancer.
As I said above, biological ageing as a ‘risk factor’ for cancer is not a new topic of study. I found an earlier article, dated 2004 and entitled, Biological ageing: A fundamental, biological link between socio-economic status and health? that describes the term as follows,
“Biological ageing is the progressive decline in physiological ability to meet demands, that occurs over time.”
Many of the references in that article are dated in the 1990s, so the topic clearly remains a ‘mystery’ to the mainstream medical establishment. The reason for this, I would suggest, is because they are not looking at cancer from the correct perspective. As the AACR article showed, the priority of the medical system is for early detection in order to initiate early ‘treatment’. Although ‘prevention’ is also mentioned, none of their suggested measures will address the issue because, again, they are starting from the wrong premise, so the ‘problem’ can never be prevented that way.
As I often emphasise in my articles and other writings, problems can only be solved or resolved by addressing the root cause. The absence of evidence that any alleged ‘infectious agent’ is a factor for cancer means, of course, that vaccinations are totally inappropriate as either solutions or preventives.
Interestingly, the 2004 article continues with the comment that,
“It is due to the accumulation of damage at the cellular level and the rate of biological ageing is determined by both environmental and genetic factors.”
I disagree that ‘genetic factors’ are involved, for reasons I’ll discuss below.
I do agree that ‘environmental factors’ are relevant, because that concept aligns with the terrain paradigm; although I would add that the phrase ‘environmental factors’ is inadequate because it fails to encompass the full spectrum of relevant factors.
The article states, under the sub-heading Why does biological ageing occur?
“ Physiological systems require constant maintenance. Maintenance requires resources.”
I agree that our bodies need maintenance.
The article also states, under the sub-heading How does biological ageing occur?
“Maintenance of physiological systems occurs primarily at the cellular level. Biological ageing is, therefore, due to the imperfect operation of maintenance mechanisms and the resultant accumulation of cellular damage. The rate at which cellular damage accumulates is determined by the balance between damage occurring and the action of defence and repair mechanisms.”
Modern medicine claims that our bodies need ‘maintenance’ in the form of pharmaceuticals, such as statins and anti-hypertensives, especially for people when they reach the age of about 50. But these, and all other pharmaceuticals, belong in the category of causal factors, not preventive factors.
However, I would agree with the general underlying message of the above statement from the article. When not maintained correctly, our bodies do accumulate damage that impairs our ability to function optimally, although ‘optimal’ will have a different meaning for each of us individually.
Unfortunately, the article includes the standard claims about the factors that influence the ability of the body to carry out maintenance,
“Both genetic and environmental factors influence the rate of biological ageing.”
I would suggest that biological ageing can be better described as the result of factors that impede the body’s self-healing processes and innate regulatory systems that serve to restore homeostasis. Anything that impedes the body’s ability to function has the ability to cause damage.
In addition, there is zero evidence that ‘genes’ determine health outcomes. Sometimes certain ‘genes’ may be found in association with certain ‘cancers’, but that does not prove causation. The BRCA1 and BRCA2 genes that are claimed to be risk factors for breast cancer provide a perfect example of this situation. Many women who have been diagnosed with breast cancer do not have either of these genes and many women who have them are not diagnosed with breast cancer. It is clearly not a direct 1:1 correlation in all cases, which means these genes cannot be considered causal factors.
The point to emphasise here is that there is no evidence that genes are causal factors of any ‘disease’. Genes - whatever they are (and that’s an article for another day) - are known to be affected by their environment, see Dr Bruce Lipton’s work on epigenetics. If genes are affected by other factors, they cannot be root causes or the initiators of anything.
Back to the effort to understand why there’s an increase in early-onset cancers.
The 2026 Nature article states,
“Identifying the full set of risk factors for early-onset cancers remains a research priority, yet is challenging. Many relevant exposures are measured incompletely across the life-course, individual effects may be modest and etiologic drivers probably occur as mixtures that co-occur and interact.”
The point to note here is the focus on ‘risk factors’ instead of causal factors. I would suggest that the reason for this focus is that if ‘risks’ can be identified, ways to address and reduce them can be developed.
But this does not represent the way our bodies actually function. It also removes our ability to have agency over our own bodies.
In the course of my research for this article, I came across the term ‘geroscience’.
Geroscience is defined on the AFAR (American Federation for Aging Research) web page What is Geroscience?
“Geroscience is the interdisciplinary field that studies the biological mechanisms of aging to understand how they drive the onset and progression of chronic diseases and age-related conditions.”
The problem is that we do not all age in the same way, which can be demonstrated by what are referred to as ‘blue zones, as discussed in a September 2025 article Living in the Blue Zone,
“According to research, Blue Zones have among the world’s highest proportions of centenarians (people who live to age 100 and older). Most residents live seven to 10 years longer than the average American. On average, they also have lower rates of chronic diseases like cancer, cardiovascular disease, diabetes, and dementia.”
Five of the main places in the world labelled ‘blue zones’ are: Okinawa, Japan; Ikaria, Greece; Sardinia, Italy; Nicoya, Costa Rica; and Loma Linda, California.
It’s interesting that one of these zones is in the US, where health is not at all the best in the world, even though healthcare in the US is more expensive than in any other country, as can be seen below.
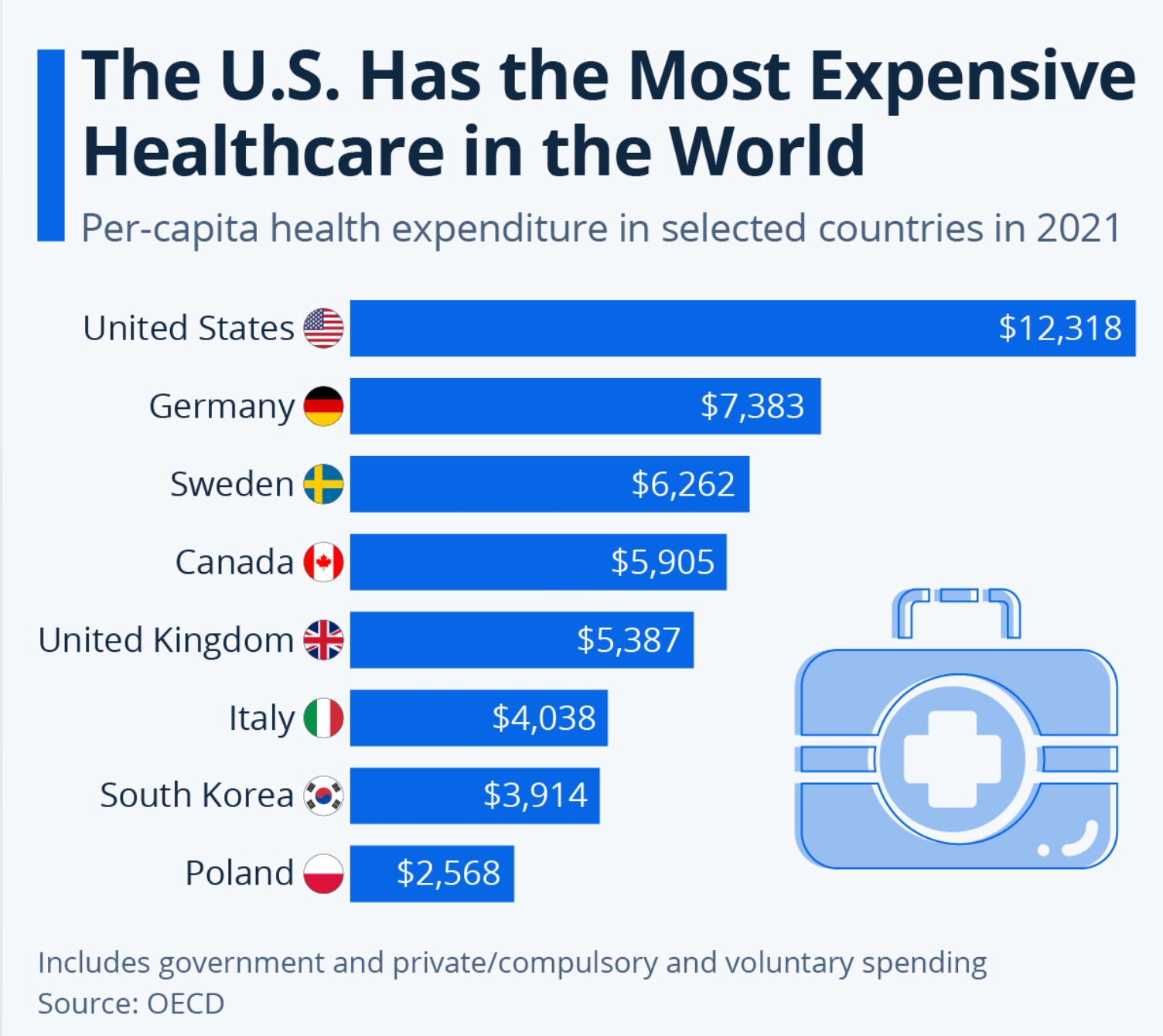
I appreciate that this is for 2021, but the difference between the US and all other countries is so huge that I doubt if the gap will have changed in the intervening years, if at all.
So how can some Americans be extremely health and live long lives, when many of then are unhealthy and have their lives shortened by various diseases?
I suspect those who live in Loma Linda, California do not subscribe to ‘modern medicine’!
Interestingly, the lifestyles of some of those people who live in ‘blue zones’ defy those described by the WHO as ‘risk factors’ for cancer; yet these people remain cancer free throughout long lives. There is definitely something else involved!
There are many facets to this topic; far too many to cover in any depth in a single article.
The key problem, as in most ‘medical research’ is that it invariably starts from the basis of faulty, if not completely flawed hypotheses and theories. Although the research may sometimes include some relevant aspects, the emphasis is always on finding ways to affect processes within the body, instead of finding ways to help support the body.
I wrote above that I have my own ideas about the reason for this situation - so here it is:
My starting point is that the body is not a machine of separate parts. Instead, it is an interconnected whole organism that is capable of self-regulation. In other words, the body has an innate intelligence and inherent abilities to support itself and its functions. Problems occur when those functions are undermined, especially, although not exclusively, through pharmaceutical interventions. Other substances that can impede the body’s ability to function optimally include the many chemical and electromagnetic influences to which it is subjected.
In addition to these ‘physical’ substances, our bodies are also influenced by non-physical influences that affect us on a mental, emotional, psychological and spiritual level. Persistent fear for example, is a known stressor that can have ‘physical’ effects. There is more than adequate evidence that these ‘non-physical’ stressors play a major role in health issues, including cancer.
I will be discussing this in more detail in future articles as well as on my podcast.
If this topic interests you, please subscribe to receive notification of future articles and podcast episodes.
Dawn 🌹
I am grateful for the kind support of paid subscribers and generous donations for coffees and/or books. [My preference is for the latter 😊]
Thank you, Dawn!
The explosion in cancers was predicted at the start of covid. Health psychology when I was an undergraduate 30 years ago could map future cancer locations. By natural disasters. Even the yearly flooding in locations near rivers. The government used psychology to implement the covid measures. They clearly would have known the fear created would raise cancers. That and the normalisation of injectables. When humans have had a survival adversion to needles and blood.